I’ve been reading ‘Pale Rider’ by Laura Spinney, a book about the Spanish Flu of 1918-19. What was learned from the Spanish Flu that we can use now? Very simple really. Historically, with an epidemic that is killing people there are three actions that work. The intention is to have the virus run out of people to infect by removing people from the virus.
Put up a ‘sanitary cordon’ that stops people entering or leaving an infected area. (eg a country’s border)
Isolate people with infection – this includes ‘social distancing’ which assumes any person could be infectious
Quarantine people who are or might be infected – includes people who cross the cordon in 1.
Success depends on how quickly and how strongly all three of these are adopted. Slow and weak/waffling gives a higher death toll (viz Italy, USA, France, UK, Spain). Quick and strong gives a lower death toll (viz maybe Australia, Hong Kong, NZ, China, South Korea, Taiwan).
Once a person has a severe infection, there appears little doctors can do – except treat secondary infections (often pneumonia) that usually do the actual killing. (See more in the analysis section below.) Doctors tend to throw the pharmacopoeia at the initial viral infection and secondary infections hoping something will work. Nurses can do a lot – especially keeping hydrated and generally looking after.
Counting
Several countries are revising counts of cases and deaths supplied to WHO. Such revision is causing a bit of finger pointing. Why?
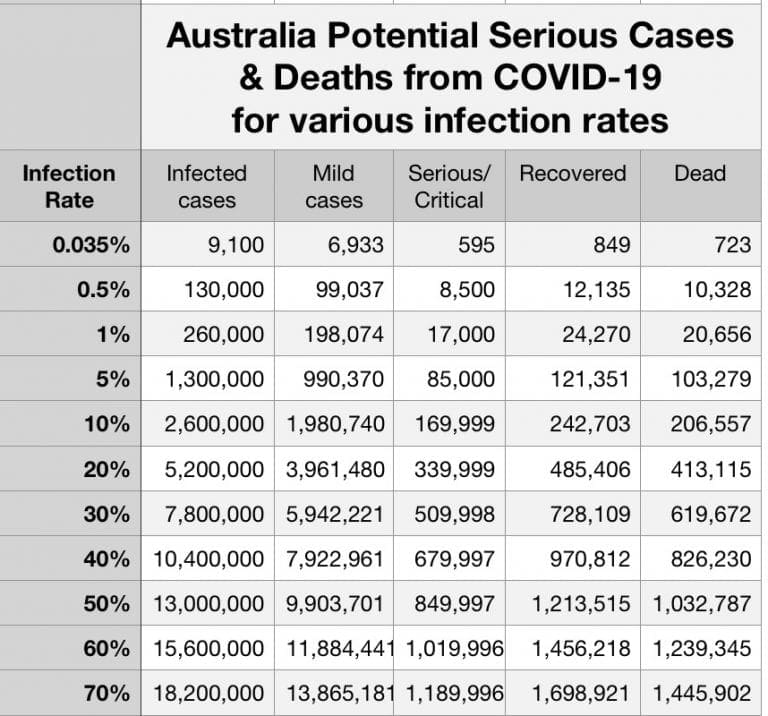
First, we know that any measurement is inaccurate and will have an estimate of its accuracy associated with it (plus or minus). In the instance of COVID counts, we know that the number of counted cases will severely underestimate the actual number because a) most people with the virus are asymptomatic; b) we usually only test people showing symptoms. Until we test every person each day, we will not know the number of cases on that day. (Even then it will only be an estimate because all tests have false positives and false negatives.) We have a similar issue with deaths. No country is recording all deaths from COVID. Some countries only count those who die in hospital (not nursing homes) and usually count only those who had tested positive to COVID before they died. So, both number of cases and number of deaths are usually under reported – and we know them with very poor accuracy.
Second, why do we care? If we spent more time and money being more precise with our measurement would that change our response. Probably not. We know that this virus is a killer disease and the three steps listed above work. Each country makes its policy accordingly. Do we really care if it kills 10% or 15% of those who show symptoms or 5% of all those infected? Would knowing accurately change our approach? Probably not. In the case of China, China has been making a song and dance about it being so successful because it has a strong central government that could shut the country down and impose very strict restrictions on its population. Many other governments have shut down their countries and imposed harsh restrictions because that appears to work. I haven’t seen that any countries have suddenly decided that on the basis of China’s success they will adopt Chinese communism.
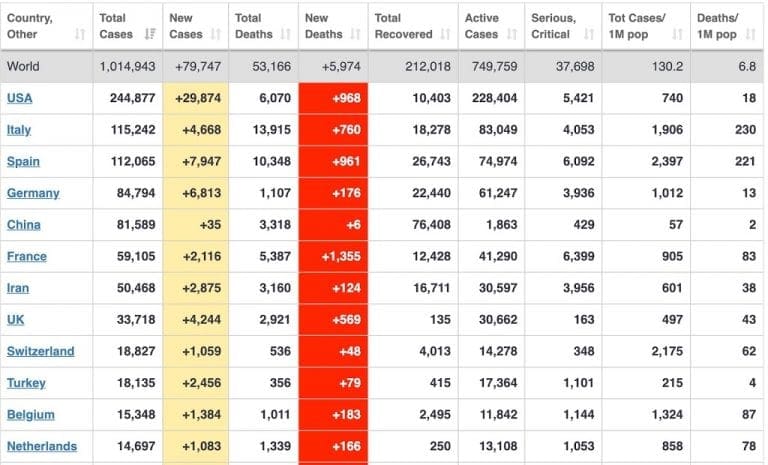
Thirdly, I did not know that this was an Olympic race with some countries winning and other countries losing. The table published by WHO is not a success table counting gold medals. Does it really matter that many countries now have more deaths than China. It is not a competition.
In the last couple of days, France has issued a completely different set of figures for numbers of cases and deaths. The UK and US keep finding more dead people when they look in nursing homes. The WHO says many countries will have to adjust their reported figures as things become clearer.
Speaking of sudden changes, it looks as though some of Wagga’s local government councillors have suddenly noticed that China has a communist government and, because of this recent change in China’s political system, decided to drop Wagga’s sister city relationship with a Chinese city. On the ball. The decision will probably be reversed when the sensible mayor comes back from sick leave.
Mutations
Why are some countries having a much higher death rate for those infected. Iceland researchers believe that there are more than 40 different mutations of SARS-COV-2 circulating and that the variety found in Italy and Austria is different to the one found in UK. Some varieties are more lethal and more than one variety has been found in the same individual – meaning the antibodies for one maybe don’t work on another. Making development of a vaccine to cover all varieties tricky. And making ridiculous the ‘herd immunity’ theory.
deCODE sequenced the virus from 643 individuals and drew a family tree of the different haplotypes found. Analysis of sequence data reveals that the haplotypes of the virus detected in the early targeted testing were almost entirely of the A2 clade originating in Austria and Italy and entering Iceland with people returning from skiing holidays. By contrast, the cases identified in the more recent targeted testing and in deCODE’s population screening show that various haplotypes of the A1 clade prevalent in countries such as the U.K. had become more common, and that there is now a wide and growing variety of haplotypes present in the population.
Data Science
Over that last 20 years statisticians around the world have teamed up with numerical analysts to be able to work through and analyse big data sets. They have even developed very robust methods of Artificial Intelligence. What can these dudes tell us that might be helpful? Let us ask Mr Google -“artificial intelligence and covid” returns quite a good haul. There are quite a few articles describing how data science can be used for i) early warnings and alerts, ii) tracking and prediction, iii) data dashboards, iv) diagnosis and prognosis, v) treatments, and cures, and vi) social control. This article published 2 April shows something of what has been published. There will undoubtedly be many red herrings, however the most likely ones will be those related to tracing – something Big Data has already shown it is good at. This one was interesting on South Korea’s use of AI – including developing a test kit and work on using AI to analyse x-rays and CT scans.
From there on, I have found the published AI and data analysis unimpressive. I think I was expecting good analysis to tell us how to treat or how to prevent a mild case becoming serious. And I found ‘not much’. Kaggle (a repository for big data sets with competitions to solve them) has several COVID sets with open challenges. (At time of writing 20 Apr, the top rated is a repository of 52,000 scholarly articles written about COVID put up by the White House to find insights about the disease and is getting a lot of action. The top Notebook leads to this plot for those who like pretties, but does not appear to have got further in a month than grouping the publications by topic of paper.) Very disappointing so far. We must make more use of AI and data analysis to help in our fight with this disease.
So far I can see that in the 100 years since the Spanish Flu, our ability to deal with killer viral pandemics has not increased much. We have advanced to the stage that we can identify the virus, give it a name and possibly develop a vaccine (in 12-18 months). But not kill the virus dead. We don’t have anything like a Dr McCoy (Star Trek) solution.
Why do some people have a worse outcome?
Why do some people get just a mild infection (possibly even asymptomatic) and some people develop severe secondary infections and die. I was hoping that good data analysis might be able to answer this question. These are examples only. I have no idea if this is useful. This paper in The Lancet discussed liver damage (very small sample sizes unfortunately). More here and here on Non-alcoholic Fatty Liver Disease.
Liver damage in patients with coronavirus infections might be directly caused by the viral infection of liver cells. Approximately 2–10% of patients with COVID-19 present with diarrhoea, and SARS-CoV-2 RNA has been detected in stool and blood samples.
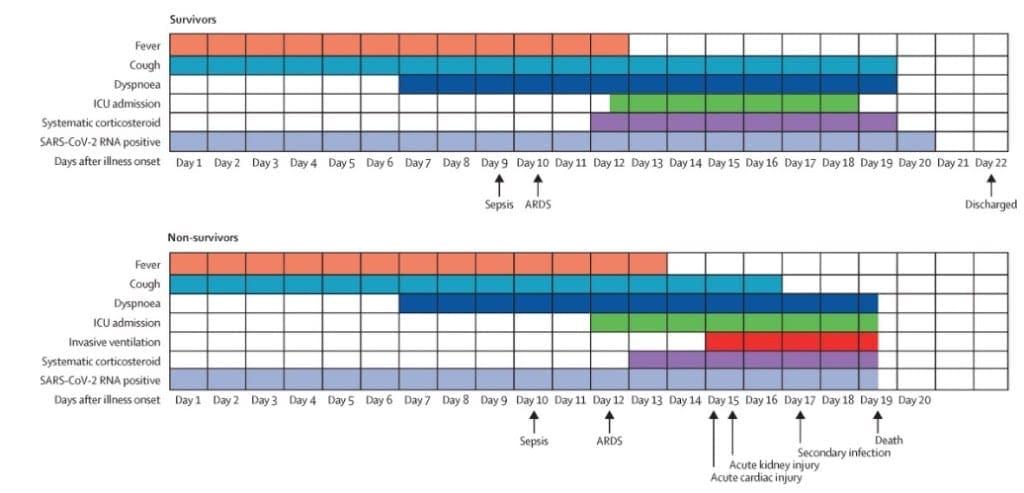
Scouring The Lancet, I found this interesting paper (published 11 Mar 2020 with small sample size). Table 1 shows that smoking or cancer are not significant indicators of survival. However, hypertension, diabetes, coronary heart disease, chronic obstructive lung disease and chronic kidney disease are all significant (the comorbidities). Quite a few laboratory tests are also significant (including the ALT listed above). Table 2 list treatments. Antibiotics and Antivirals don’t work (p-value much > 0.05) but many treatments did work. As indicators of outcome, events such as heart failure, respiratory failure, septic shock had a significant effect on the outcome as did some clinical path indicators such as ‘being admitted to ICU’, ‘how long the person stayed in hospital’ and ‘the time they were ill’. I liked the following graph. If you had a sepsis event a day late and an Acute Respiratory Distress Syndrome ARDS event two days late, you were on the wrong track.
Figure 2 has a set of interesting graphs that show blood tests of survivors and non-survivors. They might be a very useful form of triage to decided who should be occupying those scarce ICU beds and ventilators. “You’ve been here 7 days and your blood markers are wrong. Out you go.”
As I said, a very early study and a small data set. Although their statistical method looks sound, I suspect they may have tried to do too much with their small data set and may have included too many variables. I would be much happier with 10 or 100 times the data to be sure of their findings. Also, given the Icelandic studies, results from Wuhan studies might not apply against virus mutations in other countries. However, it does provide a guide. I wonder what more up-to-date studies and studies with very large data sets from multiple studies will tell us. We might have to wait.
Learning from others
I think what surprises me most in this pandemic (though it shouldn’t) is the reluctance of countries to learn from each other. Especially the west learning from the east. Arrogance. It certainly looks as though South Korea and China made a considerable amount of information available that the west has had to go and find all over again while denying the information was there. And finger pointing that they ‘weren’t told’.
My comment also refers to the complete unpreparedness of the west. Hands on hips watching China struggle with the epidemic. Australia even sold ventilators to China. We knew we would not need them. Then, a month or so later, it came as a surprise that we need hundreds of millions of masks and PPE and thousands of ventilators. Did we even think we might need them when our turn came. Arrogance that has cost many lives in Europe and US – none of which appear to have made any preparation. Followed by the inevitable blame game.
Waves
The Spanish flu had three distinct waves. The virus managed to mutate just enough that the second wave could reinfect people who had the virus in the first wave. The second wave was by far the most deadly – killing between 50 million and 100 million people and in some countries 1 in 5 people.
When our political and health spokespersons talk about a ‘second wave’, they are not talking about the Spanish Flu experience. They are talking of a re-emergence of the same virus as a consequence of removing the lockdown too early and the same virus suddenly finding more people to infect.
Contact tracing
This short video explains what contact tracing is about. Many countries (China, Singapore, Germany, Canada, South Korea, Taiwan, Ireland, UK, USA, Iceland) have used/are building/are using tracing apps such as TraceTogether or the Apple-Google app. Looks like a good idea. Will 60% of the population use it? The same arguments (social good vs hacking, privacy) are used everywhere. I do find the argument ‘against’ strange given the plethora of free apps people download to their smart phone with no concern for how their data is used or sold by the app developer. Also this wiki for a comprehensive write up.
After
From experience with Spanish Flu, we cannot expect an immediate rebound when the pandemic has played itself out. After the Spanish Flu, the world did not return to ‘normal’.
Extensive post-viral ‘chronic fatigue syndrome’ and lethargy meant that many countries went on hold for a few of years. In many cases, crops unplanted or unharvested followed by famine.
People who were infected – even mildly, never regained their health.
Many survivors developed a ‘sleepy’ sickness – a zombie like state that lasted for months.
Survivors were also melancholic and depressed – unable to work.
I understand that many people doubt that COVID-19 is as serious as the media is making out. That it is…
Shield Shrimp
When it rains across Australia’s vast inland region, temporary pools crop up all over the arid ground, giving life to a strange desert crustacean known as the shield shrimp (Triops australiensis).
Named after the formidable carapace that shields its head and upper body, T. australiensis can grow up to 7.6 cm long, and it uses its long, segmented tail and mass of 60 or so legs to propel itself through shallow water.
It also breathes through these legs – its sub-class Branchiopoda means ‘gill-legged’ – and in the females these legs bear ovisacs for carrying their tiny eggs.
Several pix in the Photo Gallery and a movie.
Acacia peuce
A rare and endangered plant. The tree grows up to 15 to 18 metres (49 to 59 ft) high, with short horizontal branches and pendulous branchlets covered in needle-like phyllodes adapted for the arid dry climate. It has a distinctive habit more similar to a sheoak or a conifer.
Although speculated to have been widespread across central Australia during wetter climates 400,000 years ago, the population is now mostly restricted to three sites, separated by the encroaching Simpson Desert. In the Northern Territory, the species is restricted to the Mac Clark (Acacia peuce) Conservation Reserve which is surrounded by a pastoral lease, Andado Station. The other two sites are near Boulia and Birdsville in Queensland. The tree is found in open arid plains that usually receive less than 150 millimetres (5.9 in) of rain per annum. They grow on shallow sand aprons overlaying gibber or clay slopes and plains and between longitudinal dunes or on alluvial flats between ephemeral watercourses.
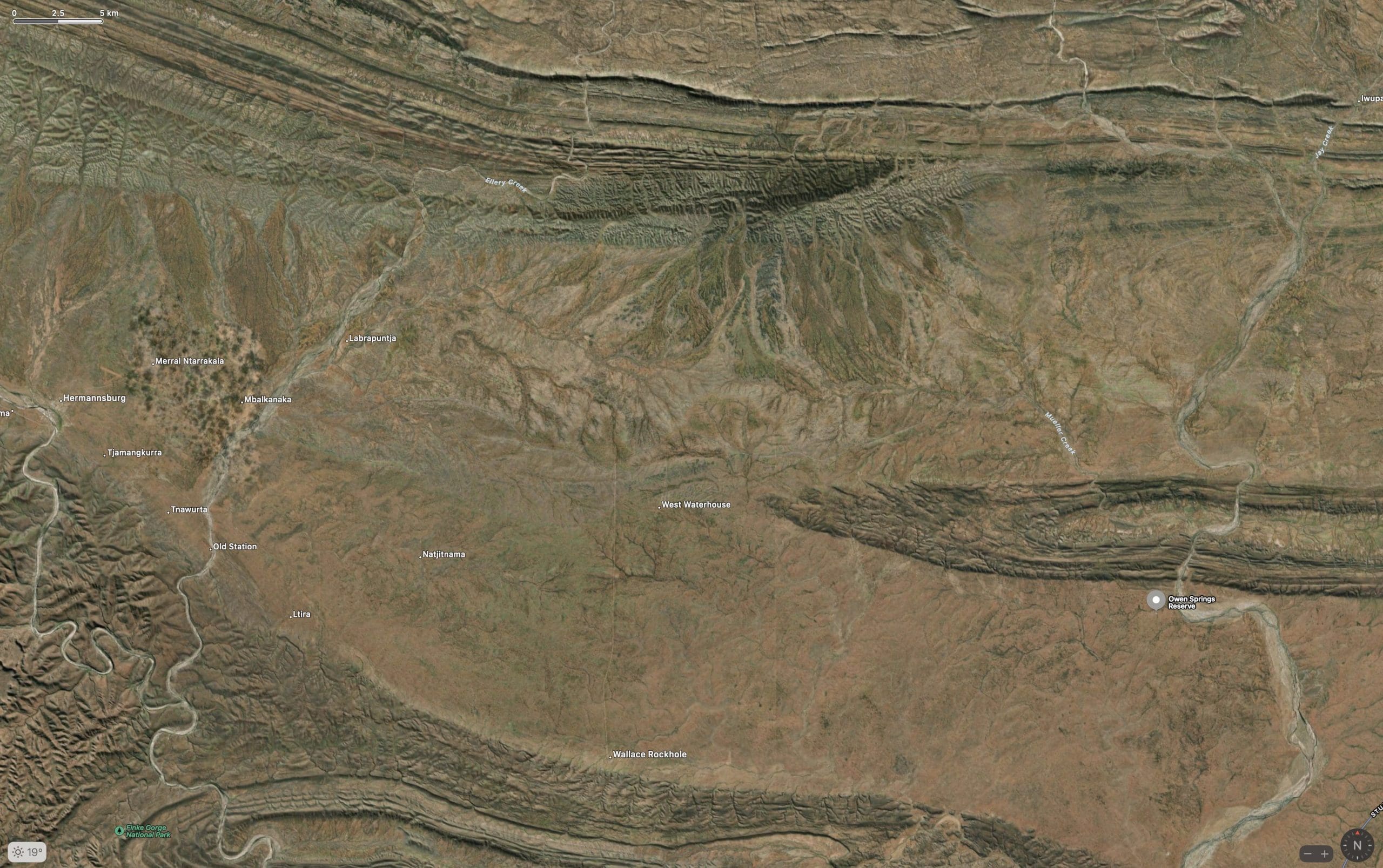
Owen Springs Reserve on Hugh River
Owen Springs was a station on the Hugh River. The Hugh River flows into the Finke (when it actually flows). Both cut through the Western MacDonnell Ranges. The image above shows Owen Springs Reserve as a dot at lower right. The river it is next to is the Hugh. Hermannsburg, our next town, is near middle left edge. Hermannsburg is almost on the Finke River. You can see both Hugh and Finke Rivers cutting through sections of MacDonnell Ranges.
Palm Valley
Palm Valley is within the Finke Gorge National Park southwest of Alice Springs. Palm Valley has a smallish population of Red Cabbage Palms (Livistona mariae). The nearest related species is 850 kilometres away in Katherine NT. The average rainfall for Palm Valley is just 200 mm per year. Small pockets of semi-permanent spring-fed pools allow the unique flora and fauna (desert fish, shield shrimps tadpoles and frogs) to survive.
It had been assumed that the cabbage palms were remnants of a prehistoric time when the climate supported tropical rainforest in what is now the arid inland of Australia. Genetic analysis published in 2012 determined that Livistona mariae at Palm Valley is actually the same species as Livistona rigida from samples collected near Katherine and Mount Isa, both around 1,000 kilometres (620 mi) away. It is now thought that aboriginal people brought the palms to here from Mataranka.
Mound Springs
Mound Springs occur around the Western edge of the Great Artesian Basin and represent a natural discharge of Artesian water that was captured many hundreds of kilometers away from rain falling along the Great Dividing Range and New Guinea. This article provides details. Dalhousie is an excellent example of a mound spring.